
Medicare
ICER seeking members for New England evidence review group

The Institute for Economic and Clinical Review (ICER) is seeking nominations for new members to the New England Comparative Effectiveness Public Advisory Council (New England CEPAC). The Council includes leading clinicians, patient and consumer advocates, methodologists, and health economists. The group holds public meetings three to four times per year to discuss evidence reports on…
Read MoreState seeking public input on 2025 health improvement plan, they are really listening

After months of the Dept. of Public Health has finalized their draft plan to set goals and strategies to improve the health of all Connecticut residents by 2025. The ambitious, detailed plan focuses on access to healthcare, economic stability, healthy food and housing, and community strength and resilience. Metrics include suicide rates, obesity, overdose deaths,…
Read MoreCost Cap underservice monitoring plan is very weak, puts people at risk
Download the report This week, the Office of Health Strategy (OHS) unveiled their plan to monitor for unintended consequences of their plan to cap healthcare cost increases. OHS acknowledged in the plan that the Cap “may cause providers to reduce provision of necessary healthcare services so as not to exceed the benchmark.” Only a very…
Read MoreCTNJ Op-Ed: Labels matter in healthcare, especially the misleading ones

The President was right – healthcare is complicated. There are lots of reasons, but a big one is language. What something is called can add to or lessen understanding. Sometimes it can be deceptive, giving the impression of a more acceptable definition than the truth. It rarely works for long, but a lot of harm…
Read MorePublic comments critical of OHS’s Cost Cap plan
Several comments submitted on the Office of Health Strategy’s plan to cap healthcare costs during the public comment period raised serious concerns. The concerns echo those raised in previous unanswered letters signed by dozens of advocates. Comments were submitted by CT legal services programs, Gaye Hyre on behalf of the advocate letter writers, and one…
Read MoreCommercial plans pay Connecticut hospitals 215% of Medicare prices, but that’s better than most states; No evidence of Medicaid or Medicare cost shifting
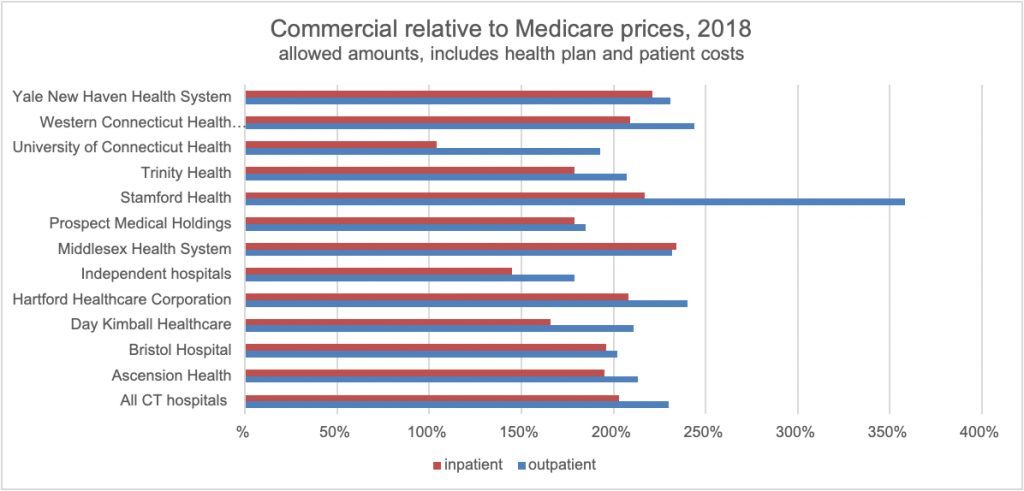
A new data set and report from RAND finds that Connecticut hospital prices paid by commercial plan were 215% of Medicare in 2018, varying from 144% for UConn Health to 282% for Stamford Health. If commercial plans had paid the same rates as Medicare that year, consumers would have saved $510 million. While high, Connecticut…
Read MoreOHS committee considers how to sell the Cost Cap to stakeholders
Last week’s meeting of the Office of Healthcare Strategy’s Cost Cap committee, as they are wrapping up the project design, ended with discussion of how to ensure their project is successful in controlling healthcare costs. Despite developing the Cap during a pandemic, there has been considerable resistance and mistrust of the concept and the process.…
Read MoreCost cap committee excludes patients’ provider choices from primary care spending increase
On Thursday, the main committee convened by the Office of Health Strategy (OHS) met to continue their work to set a cap on how much healthcare costs can increase and, at the same time, double spending on primary care. At the meeting they codified a narrow definition of primary care provider for purposes of calculating…
Read MoreCost Cap committee considers who qualifies for increased primary care spending
In response to stakeholder feedback that the prior Cost Cap levels were unrealistic and risk unintended harm to patients, at their last meeting the Office of Health Strategy’s Cost Cap committee slightly softened the cap levels. The committee continued their discussion of which providers qualify as primary care providers. OHS wants to significantly increase the…
Read MoreCost cap project sets limits on healthcare spending without public input, ignoring pandemic impact
In meetings of the committee setting limits on healthcare spending for all Connecticut residents, it appears the advocates’ sign on letter and detailed concerns about the Office of Health Strategy’s (OHS’s) Cost Cap project were not heard. The plan is being developed by a Technical Advisory Team, with members chosen only by OHS, including some…
Read More